Home »
Blogs
»
Pune: Epidemiological and Serological Surveillance of COVID-19
Pune: Epidemiological and Serological Surveillance of COVID-19
January 5, 2021
Author:
Anita_Kane
Problem/Challenge
Global data suggests that a significant proportion of SARS-CoV-2 infections are asymptomatic and remain undetected unless populations are actively screened. Understanding the extent of infection in the population permits better understanding of the severity of COVID-19 and transmission dynamics. Serological testing for antibodies against SARS-CoV-2 in a representative sample population can estimate the cumulative incidence of infection in the population. In Pune as well, there was a significant proportion of undetected cases of asymptomatic SARS-CoV-2 infections due to absence of active screening mechanism. It was thus decided to conduct a survey to understand the spread. The study was undertaken to initiate generation of unbiased data important for gaining insights into the spread of the pandemic in Pune city, and estimated the seroprevalence of antibodies against SARS-CoV-2 in five high-incidence prabhags (subawards). The survey was conducted jointly by the Indian Institute of Science Education & Research (IISER), Pune, along with the Pune Municipal Corporation (PMC), Savitribai Phule Pune University (SPPU), Translational Health Science & Technology Institute (THSTI), Faridabad, and the Christian Medical College, Vellore.
- Data was collected, stored and analysed to establish a robust testing strategy
- Better preparedness in terms of testing strategy and early detection of cases
- Early detection of cases leading to less severity and faster response mechanism thus curbing the spread in the city
Serological Testing and and Analysis of Survey Data
- Serological Testing: The study team visited selected households and briefed the occupants about the survey objectives and procedures. Blood was collected after obtaining written consent.
- SARS-CoV-2 antibody detection: IgG antibodies against the receptor-binding domain (RBD) of the viral spike protein was detected using the highly specific (100%) and sensitive (84.7%) THSTI-RBD-ELISA assay. This assay has been extensively characterised and compared with other commercially available tests for SARS-CoV-2 IgG
- Study period: Samples collected between 20th July – 5th August 2020.
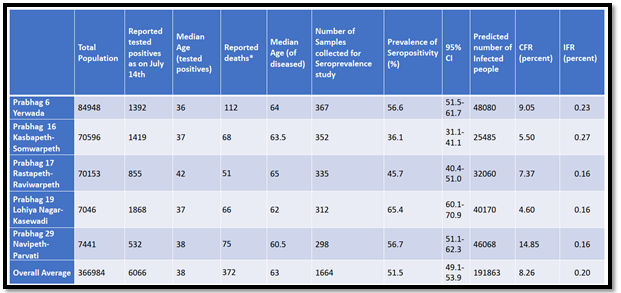
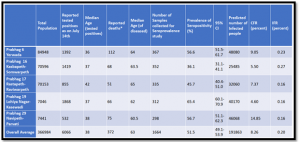
- Study settings: The PMC administrative prabhags were divided into 3 strata; high-incidence strata (incidence >0.20%), medium-incidence (between 0.10% to 0.19%) and low-incidence (<0.10%) based on the cumulative incidence of confirmed COVID-19 cases by 01 June 2020 (based on granular data provided by PMC). 5 prabhags were randomly chosen from the high-incidence strata. The selected prabhags were Yerwada, Lohiyanagar-Kasewadi, Rastapeth-Ravivarpeth, Kasbapeth -Somwarpeth, Navipeth-Parvati.
- Sample size calculation: Assuming 5% seroprevalence, the study needed to recruit 1520 individuals to obtain a 95% Confidence Interval of +/- 1% after incorporating a design effect of 2.5 for the clustered sampling design. The study recruited 1,664 individuals in the 5 selected prabhags.
- Sampling Strategy: An independent team of geospatial experts randomly selected 63 of 235 polygons with roughly equal area covering the selected prabhags. The survey team started at the centre of the grid and collected samples from every fifth house. Every fifth home was sequentially selected in multi-occupancy tenement buildings. The study included all types of dwellings; hutments, tenements, apartments, bungalows falling within the selected grid. One adult individual was selected from each household using a matrix to ensure appropriate age/gender balance. Consenting adults (≥ 18 years) from residential areas who self-reported no known acute illness at the time of collection were included in the study. No sampling was done in active containment zones.
- Sample collection: The study team visited selected households and briefed the occupants about the survey objectives and procedures. Blood was collected after obtaining written consent.
- Results: A substantive proportion of population in the five prabhags sampled in this study have been previously infected by SARS Cov-2. This indicates there has been extensive spread of infection in these prabhags.
Data Visualizations
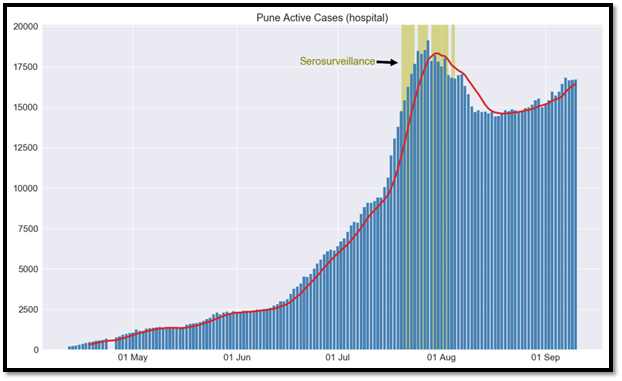
- Number of active cases is somewhat stagnated suggesting that we are adding as many new cases as they are recovering. This is an indication that inevitably, as predicted, the cases may start falling from the end of this month.
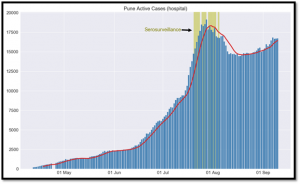
Fig 1: Prevalence of Pandemic in Pune
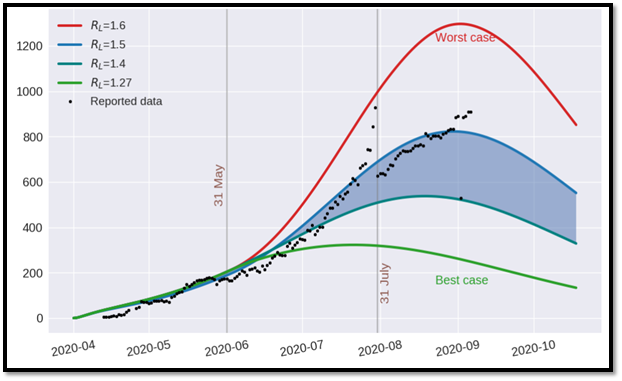
- As it is difficult to hide critical conditions, people invariably come and get themselves admitted in a Covid-19 hospital. This gives better estimation of how the disease is spreading. Trends suggest that cases may start falling from the end of this month.
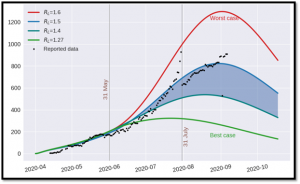
Fig 2 : Forecast of Critical Active Cases
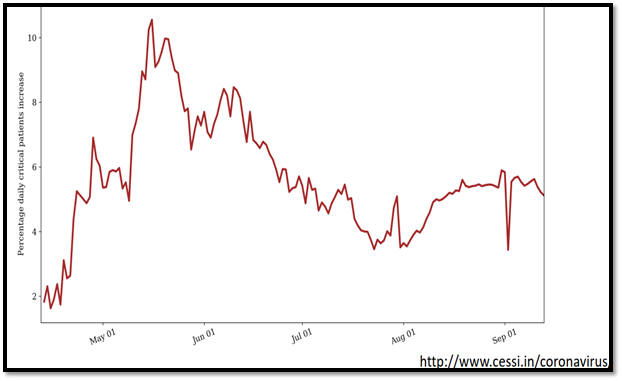
- Proportion of critical care patients is decreasing with increased number of cases. Again, corroborates that by testing more, we would not add much burden on the hospital needs, instead we would reduce the spread.
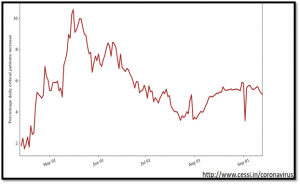
Fig 3: Percentage increase of Critical Patients
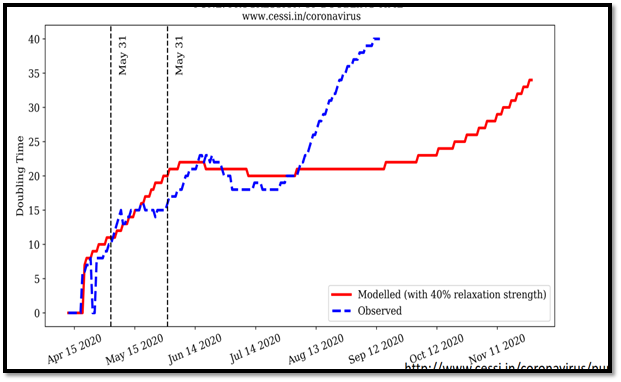
- Forecasting suggests that, Pune is doing better than expected. Case doubling is below the expectations at current level of relaxation.
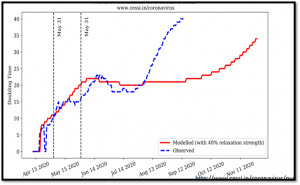
Fig 4: Progression of Doubling Time
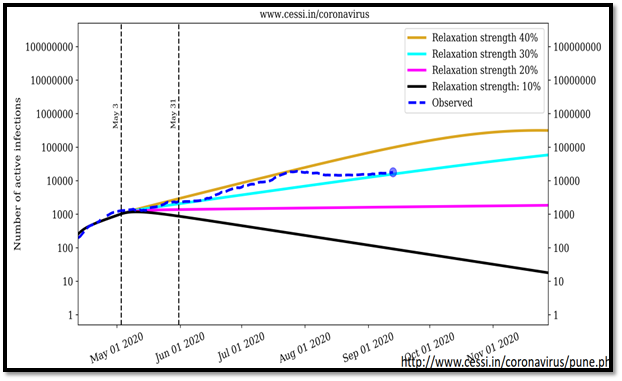
- Forecasting suggests that, Pune is doing better than expected. Increase in cases is below the expectations at current level of relaxation.
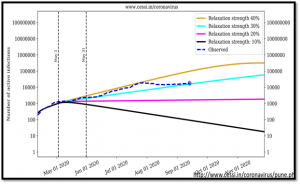
Fig 5: Progression of Infection
Conclusion
- Seroprevalence indicates that asymptomatic cases are much higher than expected, chances that an infection would lead to a disease is less than 1% and disease to death is around 0.20%. This should make people not afraid of getting tested and so that positives are isolated.
- Unless someone is critical, all should be encouraged home quarantine irrespective of the dwelling type. Educating the neighbours how-to live-in proximity of a Covid-19-positive person without getting infected themselves will help. This reduces the load on Covid-19 care centres and overall health care system.
- Time spent on hospitalization before death in Pune is less than 9, whereas national average is around 15. Educating people with symptoms like breathlessness to report to the healthcare workers is important to save lives by early hospitalization.
- While median age of infection is 38, median age of death is 63. Interestingly, older people are less affected suggesting that some levels of measures people are taking. We need to enhance this awareness.
- As community spreading is rampant (as indicated by the seroprevalence), focus should be to protect vulnerable people. Most important is to prevent large public gatherings for social, political or religious reasons.
- We cannot achieve herd immunity at the level of a large city such as Pune. People are not living as closed communities. Even if 90% of a population is already infected, remaining 10% may get infected by the people outside their locality who will bring the virus.
- It is time to bring back the economy, livelihoods by opening the city gradually.
 GOVERNMENT
OF INDIA
GOVERNMENT
OF INDIA